From SAINT to AINT


The day targeting stopped being a guess
The AINT trial came out yesterday in JAMA Psychiatry. Five years ago, a Stanford protocol called SAINT — Stanford Accelerated Intelligent Neuromodulation Therapy — compressed weeks of magnetic brain stimulation into a single week and produced remission rates that made the whole field sit up. The open-label cohort reported extraordinary early results, and the double-blind randomized trial that followed — Stanford Neuromodulation Therapy, or SNT — confirmed them. AINT is its successor and, more to the point, its examiner: the trial designed to find out which ingredient in that recipe was actually doing the work. It is a homely little name for a serious piece of science, and it carries a serious double meaning. Because for most of the history of this treatment, we aimed it with a tape measure — and the question AINT finally answers is whether that ain't good enough.
To see why this matters, you have to appreciate how strange the status quo was.
Transcranial magnetic stimulation — TMS — treats depression by holding an electromagnetic coil against the scalp and delivering rapid magnetic pulses that induce a small electrical current in the cortex beneath. It has been FDA-cleared for major depression since 2008, and it is one of the genuine successes of modern psychiatry: noninvasive, well tolerated, and effective for many people who have run out of other options. It worked. It worked well enough to build clinics around — well enough to have saved lives and changed the world for a great many people who had nowhere else to turn.
For all that, almost nobody knew exactly where on a given person's brain the coil should go. The dominant method, proposed back in 1995, was essentially a rule of thumb: find the spot that twitches the thumb, then move a fixed distance forward along the scalp. A popular later method moved that forward about a centimeter. A tape measure. The same directions for everyone.
Think about what that assumes. It assumes that very approximate directions are good enough. Imagine telling an Uber driver that your destination is "about five miles south of here."
More than a decade ago, Michael Fox and colleagues suggesting something different: that the TMS sites that worked best for depression shared a signature and sat on regions of prefrontal cortex whose activity ran opposite to a deep mood-regulating hub called the subgenual cingulate. But was this fMRI targeting approach better? The alternative is to use each person's own functional MRI scan to find their circuit — the brain's equivalent of GPS routed to a specific address rather than an average one. It was a generic map versus a personalized one.
The tape measure approach is not necessarily wrong; it's just sometimes spot on and sometimes quite a distance from where you actually want to go. The relevant circuitry sits in different places in different people, so a single generic instruction will land beautifully for some and miss the address entirely for others. Or at least that's what some of us believed. Others in the field thought that the thing being targeted was big enough, like "downtown" of a city, or a large music festival, that the "five miles south" instruction was more than sufficient. So the stage was set for the study. How much was precision and personalization worth?
And that question was genuinely open because SAINT and SNT had changed several things at once. It used individualized imaging to pick the target, and an accelerated schedule, and a high dose, and multiple sessions a day. Maybe the magic was the targeting. Maybe it was the dose. Maybe it was simply doing two months of treatment in a week. No one could say, because the experiment that would pull those threads apart had not yet been run.
Before the study, we had clues about how this study would turn out.
Because the tape measure lands in slightly different spots in different people, you can run a kind of natural experiment after the fact: gather patients who were all tape-measure targeted and, because of the imprecision of the tape measure, there is an effectively randomized point cloud of targets that are sometimes spot-on with the functional target and sometimes quite a distance away. A careful review by Robin Cash and Andrew Zalesky in 2023 showed that in these incidental stimulation studies, the closer you got to the functional target, the better you did across 4 independent datasets.

Even before the incidental studies, I personally had a strong intuition that where you stimulate a system this intricate could not possibly be a rounding error. So at our clinic we began offering fMRI-guided accelerated TMS clinically in 2021, among the first groups in the country to do so, for patients willing to try it before the randomized evidence existed. To my knowledge, Acacia has treated more people with accelerated fMRI-guided TMS than anywhere else in the world including places like Stanford and Harvard. Over the years, I've watched people who had been ill for years come back to life after a five-day treatment.
Once the incidental studies started coming out, I was completely convinced in the superiority. But nothing beats a head-to-head randomized trial.
That is what Joseph Taylor and his colleagues built.
The design was clean: Forty adults with moderate-to-severe treatment-resistant depression, ages 22 to 80. Each got a functional MRI scan up front. Then each was randomized to receive accelerated TMS aimed in one of two ways: at their individualized, connectivity-based target, or at a conventional scalp-based target. Everything else was held identical — the same 1,800 pulses per session, ten sessions a day for five days, real-time neuronavigation keeping the coil precisely on target throughout. The only thing that differed between the two groups was where, on each person's individual cortex, that target sat. Participants and clinical raters were blinded to which group they were in.
So, after a decade and a half of debate, who was right?
Drumroll please...
The fMRI group won. By a lot.
The headline numbers: 80 percent got better in the fMRI targeted group vs 60 percent with scalp-based targeting. Same machine, same dose, same week, same everything. Twenty points of difference, bought with nothing but a better-chosen address. Sometimes we quantify things with a term called "number needed to treat" for benefit. Here, it's a number needed to scan: how many people do you have to scan before you get an extra response? The answer? 5. If you do 5 scans, you get one additional person better. That's really good. Remember, smaller is better for this number and 5 is superb for this population. For comparison, one of the most successful drugs this decade has been esketamine (Spravato) with an number needed to treat of ~7. In the US, we've spent about ~$4,000,000,000 on the drug alone, and at least as much on top of that on the doctors and facilities administering it.
All the usual caveats apply: this was a small trial: forty people, at a single site, without a sham arm (although remember that the FDA clearance for SNT was based on n=29... big effect sizes mean smaller studies work). The authors are already planning a larger, multi-site study to confirm it across more diverse patients and to track the longer-term effects.
What blew me away was not just Joe's number. It was how closely it aligned with everything that had come before. Three different methods, sharing almost none of the same weaknesses, have now landed on nearly the same number.
The first is AINT itself: a randomized trial, the gold standard for causation, showing a twenty-point gap.
The second is our own clinic's data. At Acacia we have been comparing patients treated with fMRI-guided neuronavigation against those treated without it. Our preprint shows a large advantage; and last month, at the Clinical TMS Society annual meeting, my colleague Danielle DeSouza presented our latest figures — roughly a twenty-point gap, 82 percent response with neuronavigation versus 60 percent without.
The third is the old incidental-targeting correlation. Take that R of around negative 0.55, square it — the share of the variance it accounts for is ~30%. As a very rough approximation, what would happen if we "subtracted" the benefit of neuronavigation by the amount suggested by the incidental studies? 80% x (1 - 30%) = 56%; or with our numbers: 82% x (1 - 30%) = 57%.
These three numbers are strikingly similar.
A randomized trial, a naturalistic clinic cohort, and an old incidental stimulation site correlation — arriving by three completely different roads at nearly identical answers. When independent approaches that share none of the same blind spots converge like that, you are about as close to "this is real" as this kind of science lets you get.
So here is the conclusion, simple enough to put on a coffee mug: TMS works, and it works better when you know where you're going.
The strongest objection deserves a fair hearing, and it runs like this. If the problem is just that the tape measure sometimes misses, why bother with an expensive scan at all? Why not get around the targeting problem with brute force — just turn up the power, or change the shape of the coil to stimulate broad and deep, flooding a wide swath of cortex so that you cannot miss? It is a reasonable instinct. If you can't aim well, spray widely.
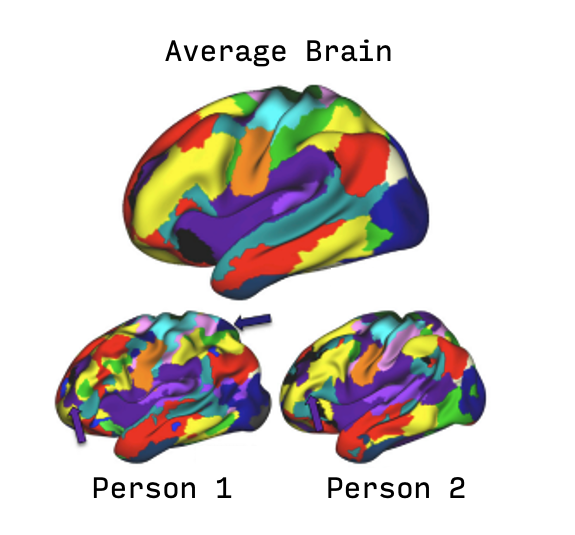
The relevant networks are not laid out the same way in everyone. In some people a broad field would do fine, because the therapeutic territory is large and contiguous. But in others the map is patchy: neighboring patches of cortex pull in opposite directions, some toward improvement and some away from it (e.g. very crudely in the picture below, Red is the default mode network which pulls in one direction and Yellow is the fronto-parietal network which pulls in the opposite direction). Flood a patchy brain with a broad, undifferentiated field and you may push in the right direction in one spot and the wrong direction right next door — and net out, on average, going nowhere. There's been ongoing debate about whether broad approaches are better, but no clear evidence that they are; brain patchiness, in my opinion, is the best explanation as to why.
None of this means fMRI is the only road to personalization. People are working hard on cheaper proxies — heart-rate and neurocardiac signals, EEG, TMS-EEG — and some may well pan out. But for now, functional-connectivity imaging is the one that has actually been put to the randomized test and passed.
Which brings me to the part of this I cannot write about coolly, though I will try to write about it justly.
The scan costs money. The accelerated protocol costs money. There is no use pretending otherwise: this is genuinely expensive — far more than a bottle of generic antidepressants, though, it is worth saying, not more than a great deal of what medicine does every day without a flicker of hesitation. Is it cost-effective? I believe the answer is yes, emphatically, and I intend to make that case rigorously in a more technical piece to come. But even the back-of-the-envelope version is stark: it is wildly more cost-effective than most of the things coming through FDA approval these days. The median list price of a newly launched American drug last year crossed $370,000 — and a fair number of the rare-disease and oncology products that drive that figure do not reliably extend life by even a year.
So the real question is not really about cost-effectiveness at all. The arithmetic is not close. The real question is the uncomfortable one underneath it: are we, as a society, willing to spend money to relieve the suffering of the depressed? Watch where the dollars actually flow, and the revealed answer is — not really.
We do not run medicine this way anywhere else. You would not ask a surgeon to operate without a scan. We would consider it not merely unwise but a species of malpractice to send a neurosurgeon, or an orthopedic surgeon, into the body blind when the technology to see exists. Of course they should have the picture. Of course the target should be found, not guessed. We grant this instantly, reflexively, everywhere the body is concerned.
And then the moment the organ in question is the brain, and the suffering is psychiatric, the instinct reverses. Suddenly the scan is a luxury. Suddenly we are asked, with a straight face, whether we can make do without it.
I understand some of how we got here. Psychiatry has spent a long time as medicine's poor relation — underfunded, a little ashamed, taught to make do and not to ask for much — while other specialties built their cathedrals of imaging and instrumentation as a matter of course. We learned to be grateful for scraps. So when something genuinely new and genuinely good finally arrives, the reflex is to apologize for wanting it badly. I think we should unlearn that reflex. Not out of grievance, but out of something closer to justice: a refusal to keep ranking psychiatric suffering beneath every other kind.
And there is a particular cruelty folded into the structure of this problem. The very illness in question — depression — attacks exactly the faculties a person would need to fight for their own coverage. It drains energy, fogs concentration, erodes memory and the capacity to make decisions, to fill out forms, to sit on hold, to file the appeal and then the second appeal. The patients least able to advocate for themselves are precisely the ones who need the treatment most. It is an unreasonable thing to ask of someone whose disease is, in part, the inability to act — and often too much even for the family standing beside them.
There is real reason for hope here, all the same. Blue Shield and a growing number of other plans have moved to cover accelerated, fMRI targeted TMS like Magnus Medical's SAINT / SNT-TMS, and there are signs more are on the way. This is the system, slowly and haltingly, doing the right thing. We should help it along as clinicians, patients, families, and anyone with a hand on a policy or a law or a budget with the insistence of people who know they are asking for something entirely reasonable and are simply done pretending otherwise.
Let me end where the science is heading.
For the rest of medicine, anatomy is not optional. We do not treat the heart, or the spine, or the abdomen as a black box to be poked from the outside and hoped at. We look. The dream — and after today it reads more like a plan than a dream — is a psychiatry in which the brain's anatomy is as ordinary a part of treatment as the body's anatomy is everywhere else: where we look before we intervene, as a matter of course, because the alternative has finally come to seem as strange as operating blind.
Today's trial did not invent that future. The work it rests on goes back decades — to the connectivity maps drawn in the early 2000s, to the Stanford lab that turned those maps into a five-day treatment, to a hundred contributions in between. But it took a clean experiment to turn a strong suspicion into being more likely true than not. For that the field owes a real debt to the trial's authors: Joseph J. Taylor, who led it, and Shan Siddiqi and Michael Fox, its co-senior authors. It is, in my opinion, the single most important papers psychiatry has produced since the SNT paper itself. Psychedelics are important, but they're an important evolution, not a revolution: broad activation of the brain, albeit more acutely and more powerfully. The AINT study is important because it's perhaps the first victorious battle in a war to make psychiatry practically and actually about the brain.
From SAINT to AINT: from a protocol that worked to the proof of why it works.
Somewhere inside the gap between sixty percent and eighty percent is a particular person — tired, out of options — for whom knowing exactly where to aim will be the difference between life and death.
That is worth a scan.